Algorithms
Western Trauma Association Algorithms
Algorithms Available Online
Click here to download published WTA Algorithms
- Management of Pelvic Fracture with Hemodynamic Instability (2008)
(1 author: James Davis, M.D.) - Management of Adult Blunt Splenic Trauma (2008)
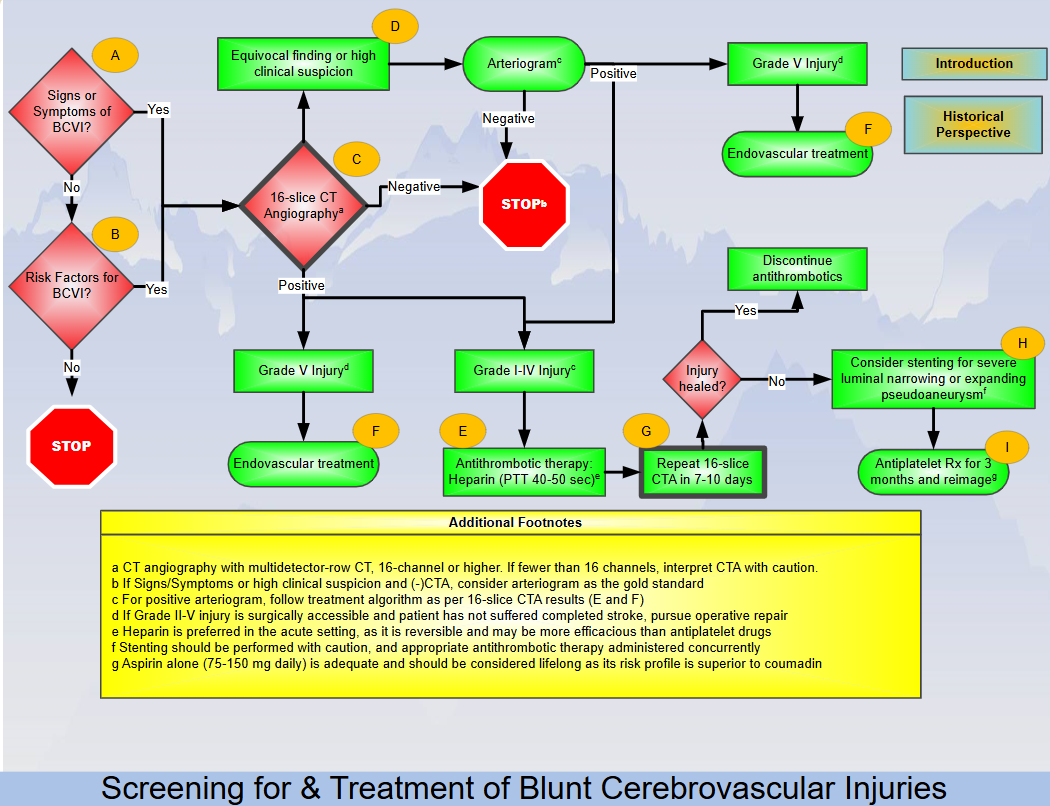
(1 author: Frederick Moore, M.D.) - Blunt Cerebrovascular Injury
(1 author: Walter Biffl, M.D.) - Nonoperative Management of Adult Blunt Hepatic Trauma
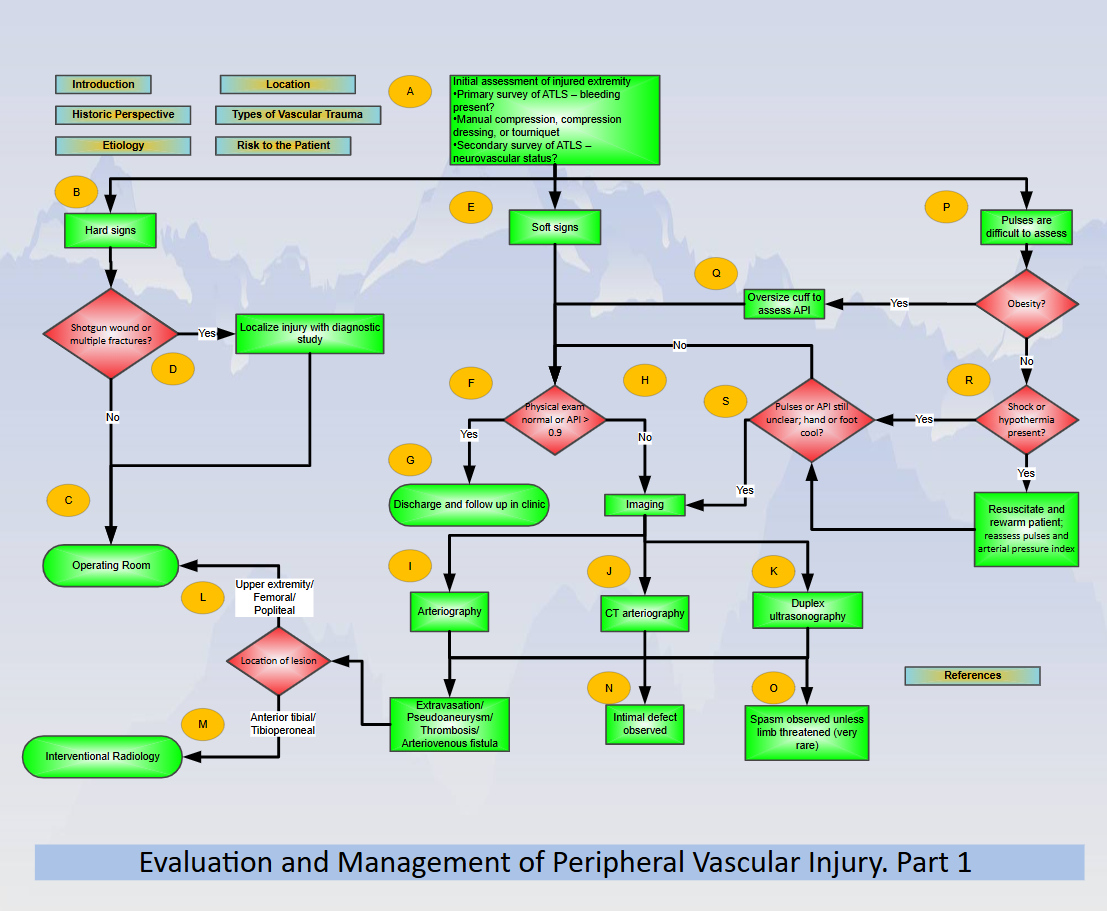
(1 author: Rosemary Kozar, M.D.) - Evaluation and Management of Peripheral Vascular Injury. Part 1.
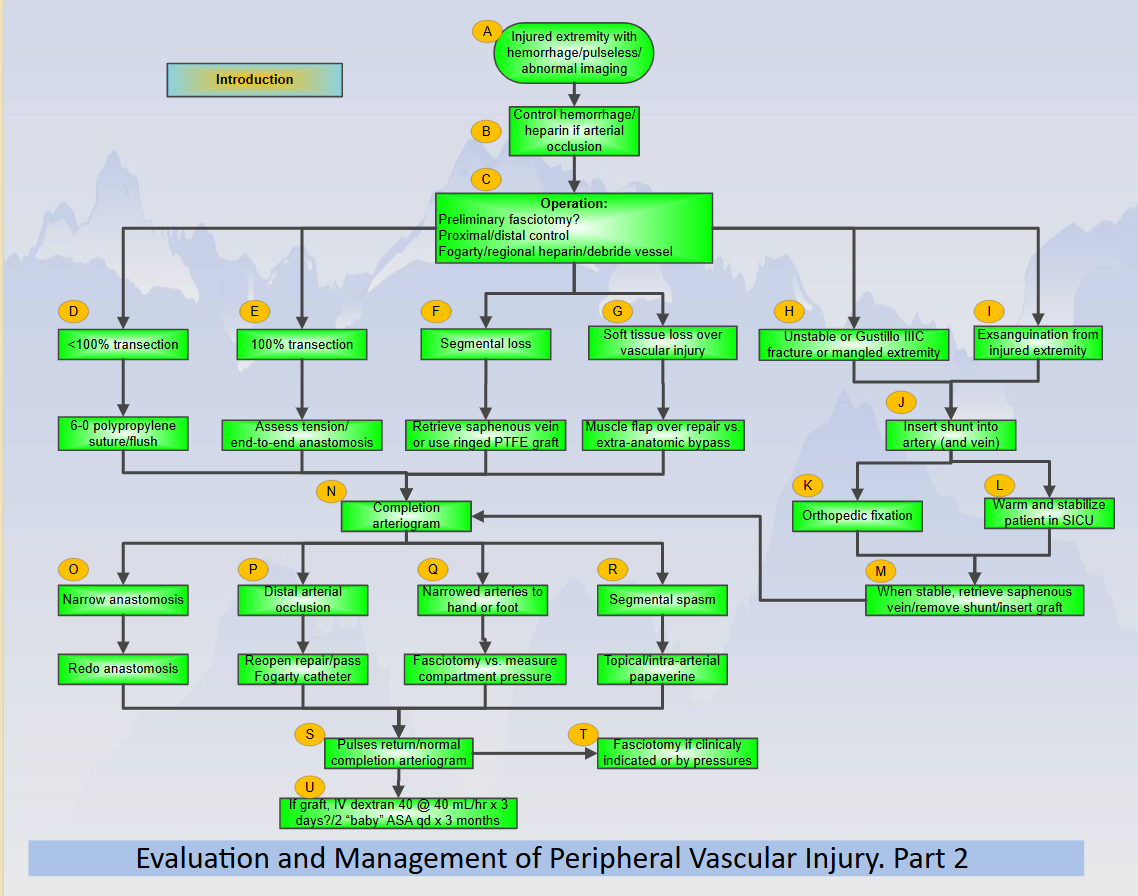
(1 author: David Feliciano, M.D.) - Evaluation and Management of Peripheral Vascular Injury. Part 2.
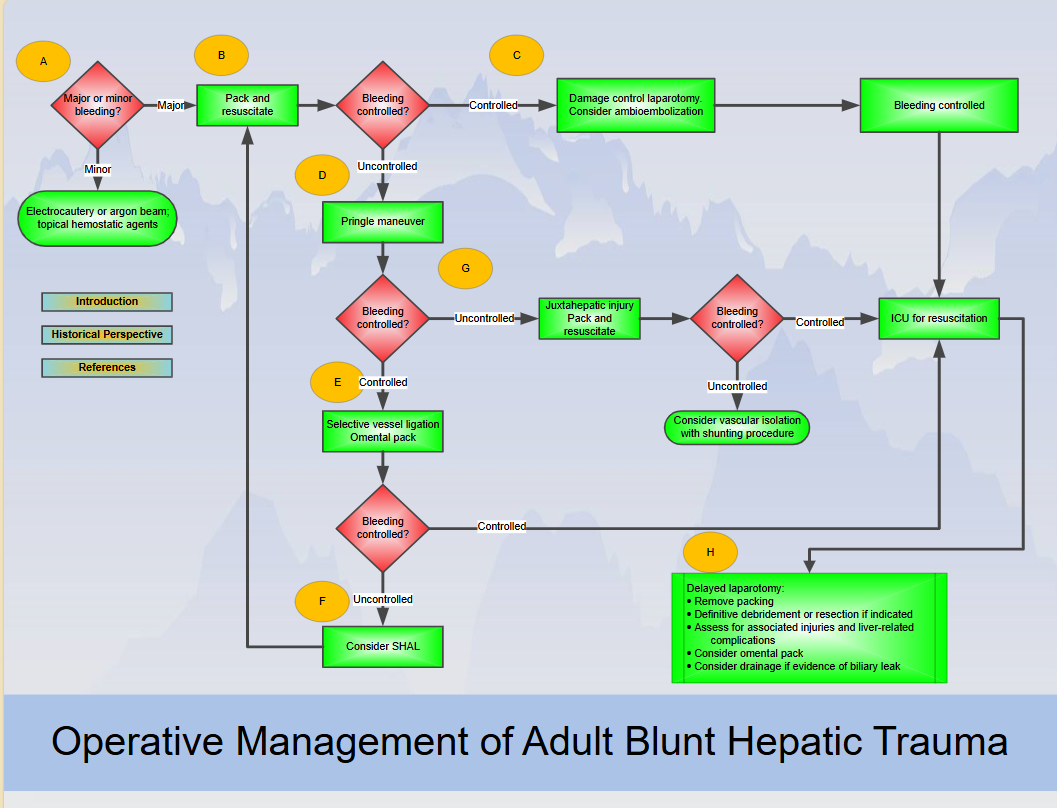
(1 author: David Feliciano, M.D.) - Operative Management of Adult Blunt Hepatic Trauma
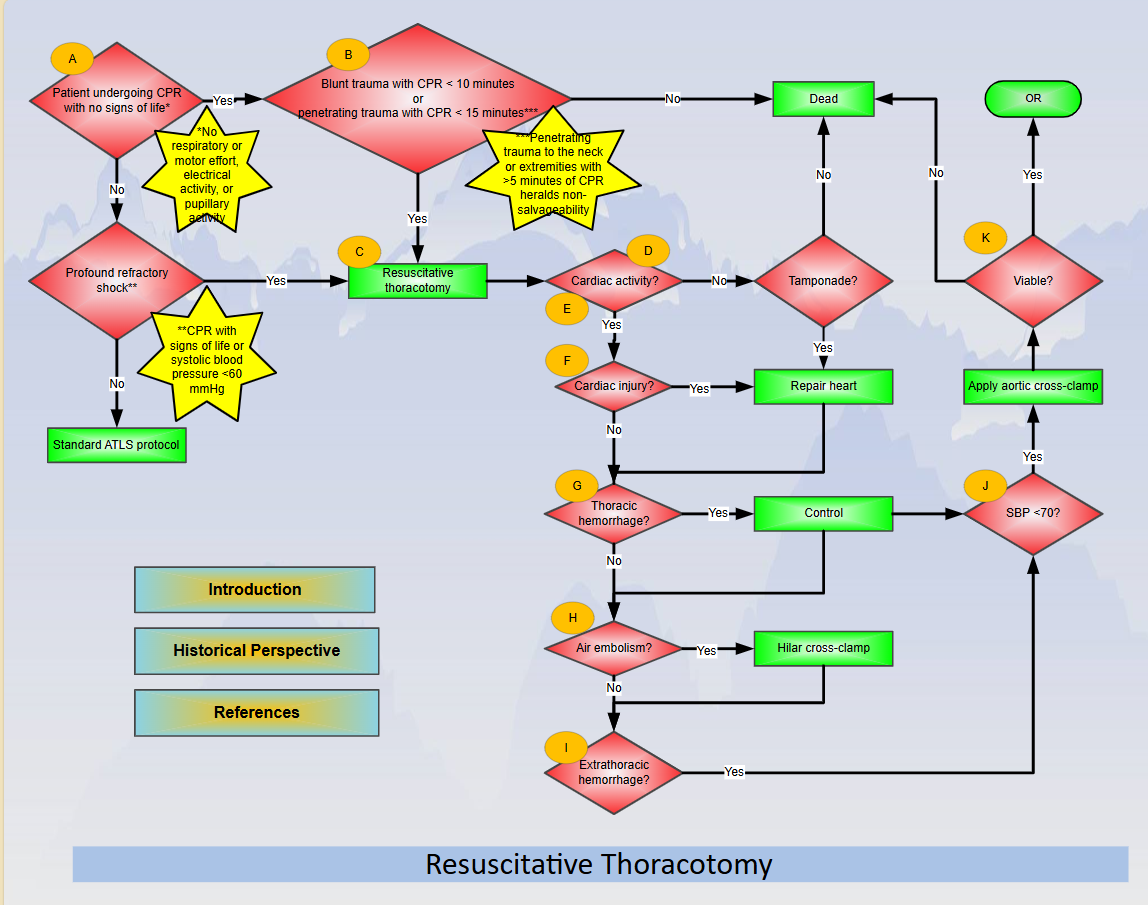
(1 author: Rosemary Kozar, M.D.) - Resuscitative Thoracotomy
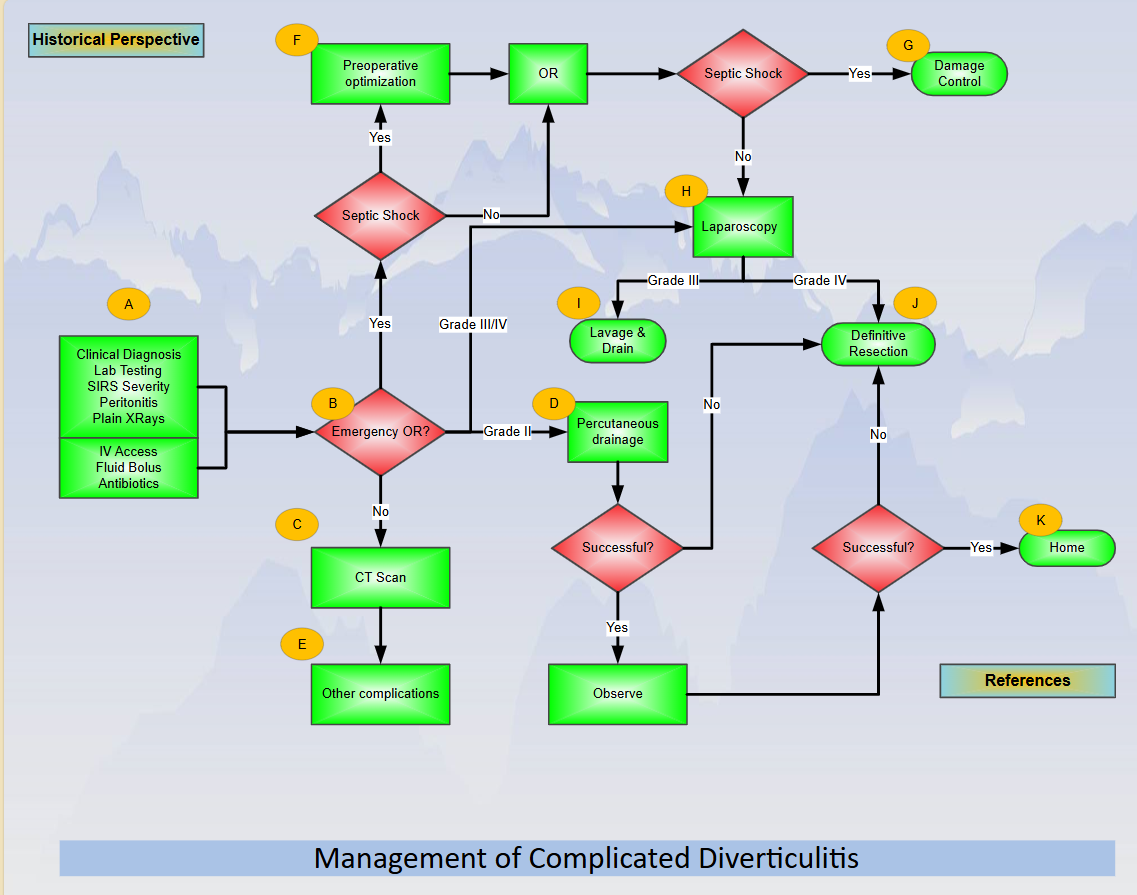
(1 author: Clay Cothren Burlew, M.D.) - Management of Complicated Diverticulitis
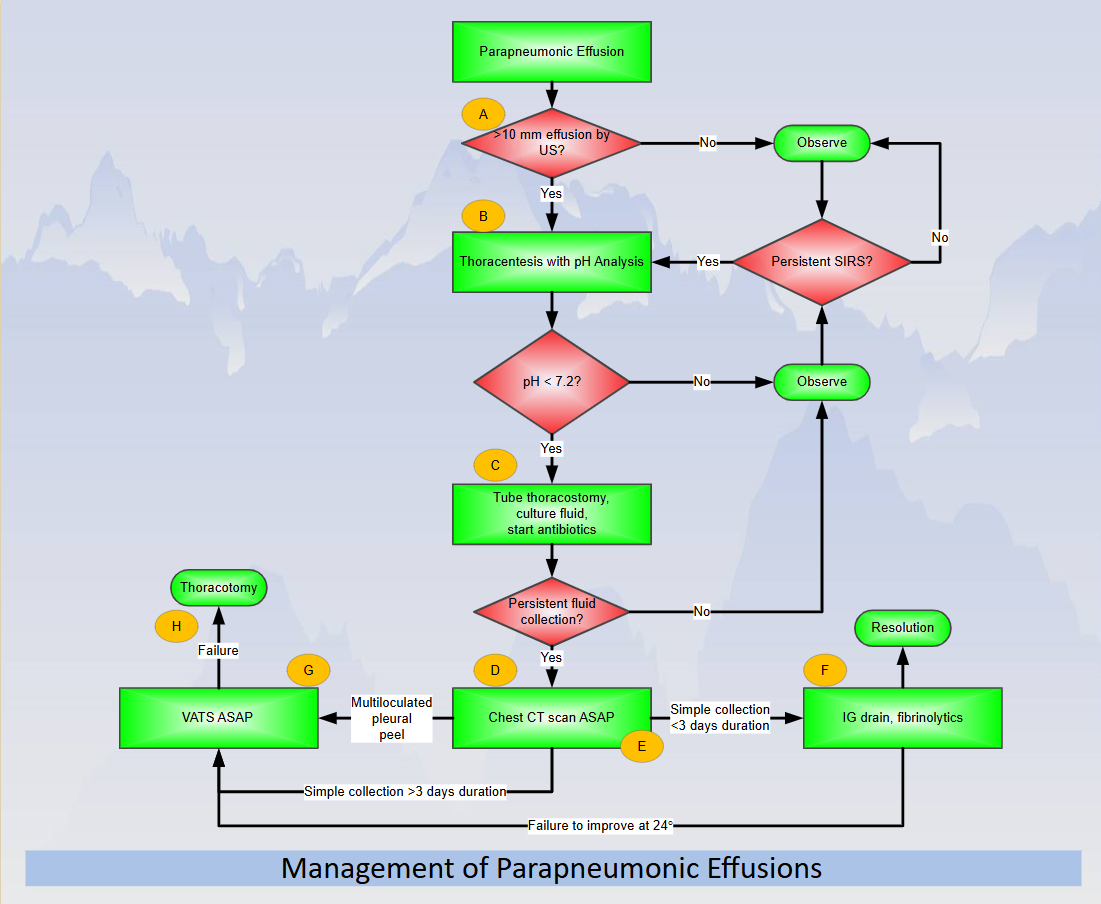
(1 author: Frederick Moore, M.D.) - Management of Parapneumonic Effusion
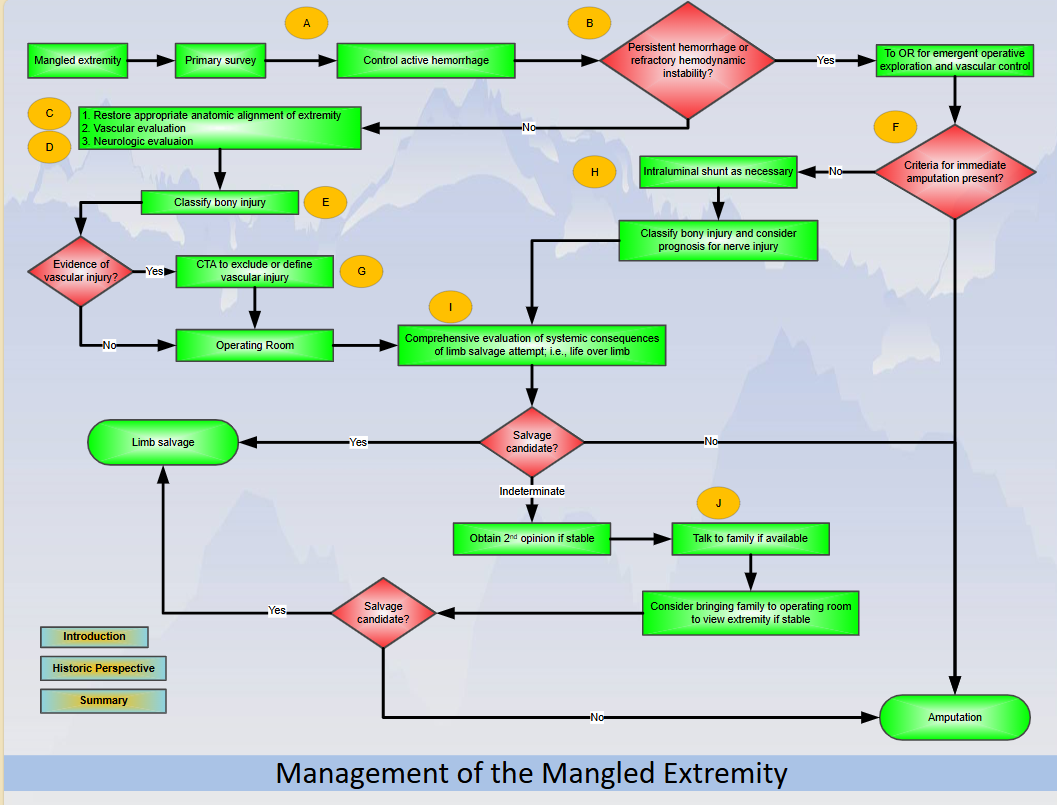
(1 author: Hunter Moore, M.D.) - Management of the Mangled Extremity
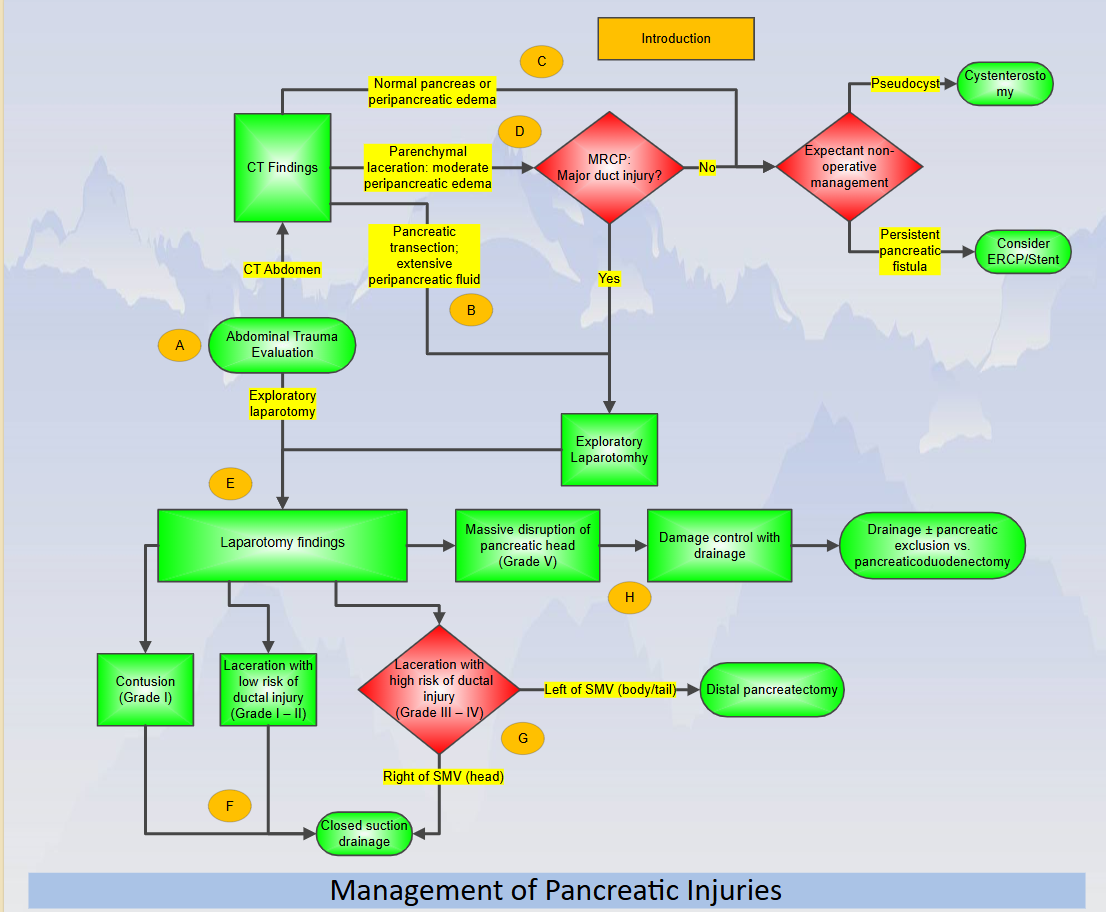
(1 author: Thomas Scalea, M.D.) - Management of Pancreatic Injuries
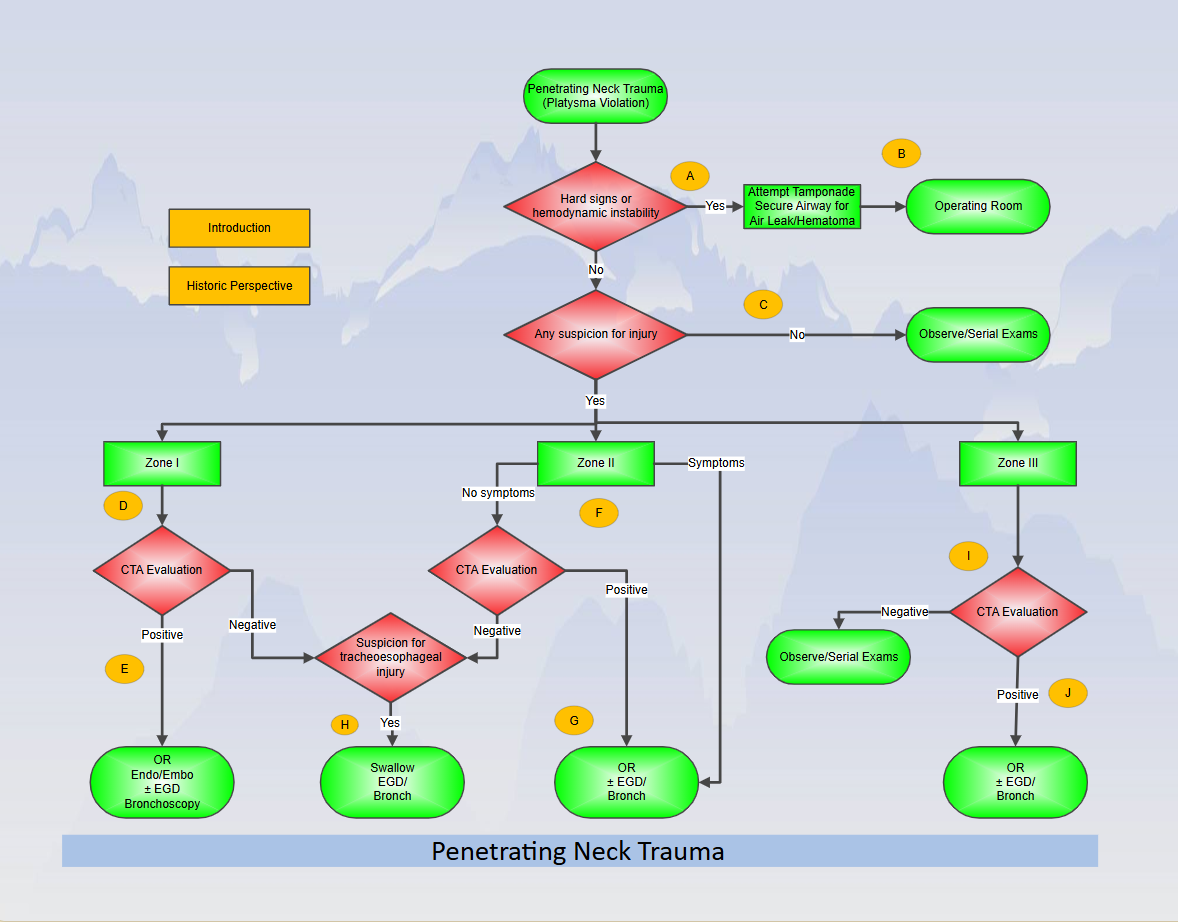
(1 author: Walt Biffl, M.D.) - Penetrating Neck Trauma
(1 author: Jason Sperry, M.D.) - Penetrating Chest Trauma
(1 author: Riyad Karmy-Jones, M.D.) - Diagnosis and Management of Esophageal Injuries
(1 author: Walt Biffl, M.D.) - Major Abdominal Vascular Trauma
(1 author: David Feliciano, M.D.) - Duodenal Injuries
(1 author: Ajai Malhotra, M.D.) - Management of Pelvic Fracture with Hemodynamic Instability (2016 Updates)
(1 author: Thai Lan Tran, M.D.) - Rib Fractures
(1 author: Karen Brasel, M.D) - Adult Blunt Splenic Trauma (Updated 2016)
(1 author: Susan Rowell, M.D.) - Colorectal Injuries
(1 author: Walt Biffl, M.D.) - Renal Injury Found on CT Scan
(1 author: Carlos Brown, M.D) - Renal Injury Found at Laparotomy
(1 author: Carlos Brown, M.D) - Abdominal Stab Wounds
(1 author: Matt Martin, M.D.) - Abdominal Gun Shot Wound
(1 author: Matt Martin, M.D.) - Open Abdomen
(1 author: Jack Sava, M.D.) - Prehospital Resuscitation
(1 author: Jason Sperry, M.D.) - Burn Patient Triage
(1 author: Gary Vercruysse, M.D) - ICP Management in TBI
(1 author: Hasan Alam, M.D.) - Cervical Spine Clearance
(1 author: David Ciesla, M.D.) - VTE Prophylaxis
(1 author: Eric Ley, M.D.) - Nutrition in the Critically Injured Patient
(1 author: Jennifer Hartwell, MD) - Blunt Hollow Viscus Injury
(1 author: Jordan Weinberg, MD) - Traumatic Hemothorax
(1 author: Marc deMoya, MD) - Traumatic Pneumothorax
(1 author: Marc deMoya, MD) - Pediatric Emergency Resuscitative Thoracotomy
(1 author: Matthew Martin, MD) - Rectal Trauma
(1 author: Morgan Schellenberg, MD) - Blunt Hepatic Trauma
(1 author: Natash Keric, MD) - Extremity Vascular Trauma
(1 author: Charles Fox, MD)
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
The Western Trauma Association Critical Decisions in Trauma ad hoc committee was born out of a call for evidence based care by our Past Presidents to aid the clinician at the point of care with a tool that could be easily accessed and implemented.1
An algorithm is an illustration of a series of medical decisions that address certain patient specific conditions outlining appropriate responses intended to lead to an outcome.2, 3 The goals of an algorithm are to identify diagnostic alternatives, treatment options, and outcomes by weighing decision benefits against risks and costs. A primary benefit of a well – developed algorithm is that it focuses the reader on the critical decision points in any clinical scenario and specifically lists the input data that leads to a decision. Algorithms can be applied to specific problems, processes, or diseases. They allow for evolution of a disease related topic with new information or clinical conditions that may affect decision making later in the time course of a situation. They can convey the scope of a clinical condition from presentation, through testing and assessment, followed by a clinical judgment and action leading to an eventual outcome. Annotations are added to appropriate points on the algorithm and are necessary for all decision nodes. The purpose of the annotation is to explain all critical factors affecting decisions in as concise a manner as possible. The primary advantage of an algorithm is that it can summarize an evidence based guideline into an easily and quickly available practice protocol for use in the clinical care setting. The Western Trauma Association has played a significant role in guiding the practice of trauma surgery based on sound scientific evidence through publication of its multi-center trials.4-8
High quality practice algorithms will further serve the trauma community by an efficient review of current recommendations in trauma decision making.
The WTA Critical Decisions in Trauma ad hoc committee oversees the development of these algorithms. After a thorough literature review, which includes review of currently published guidelines, a draft document is distributed to the committee. Critical review by the committee members is used to develop a second draft. The algorithm is reviewed and revised at a meeting of the committee. The algorithms are presented to the WTA membership at the Annual Meeting. Membership discussion results in further refinement before final submission to the Journal of Trauma and publication on the website.
We anticipate that implementation of the algorithms will require consideration of institution specific capability. An additional benefit of algorithm development is to reveal areas of uncertainty thereby defining the grey areas.1
These areas are perfect questions to be developed into clinical research projects. Algorithms will be forwarded to the WTA Multi-institutional Trials Committee for consideration of study development to test application of the algorithm. Further, a study group may be formed to perform decision analysis if appropriate for the given question.9 Each algorithm will be reviewed on a cycle of every three years by the steering committee. If substantial revision is necessary the algorithm may be directed back to the expert panel for revision. These algorithms exist in a series to follow and we look forward to the trauma community testing the algorithms and further refining care by eliminating the grey areas in decision making.
References
1. Moore FA. Evidence-based medical information technology: the next generation. J Trauma 2007; 63(6):1195-205.
2. McIntyre RC, Jr., Stiegmann G, Eiseman B. Surgical Decision Making. 5th ed. Philadelphia, Pennsylvania: Elsevier Sanders, 2004.
3. Moore E, Eiseman B, Van Way C. Critical Decisions in Trauma: Mosby, 1984.
4. Biffl W, Cothren C, Brasel KJ, et al. A prospective observation study of the optimal management of patients with anterior abdominal stab wounds. J Trauma 2008:in review.
5. Cogbill T, CC C, MK A, et al. Management of severe hemorrhage asscoaited with maxillofacial injuries: A multicenter perspective. J Trauma 2008; 65:994-999.
6. Karmy-Jones R, Nathens A, Jurkovich GJ, et al. Urgent and emergent thoracotomy for penetrating chest trauma. J Trauma 2004; 56(3):664-8; discussion 668-9.
7. Livingston DH, Lavery RF, Mosenthal AC, et al. Recovery at one year following isolated traumatic brain injury: a Western Trauma Association prospective multicenter trial. J Trauma 2005; 59(6):1298-304; discussion 1304.
8. Rozycki GS, Knudson MM, Shackford SR, Dicker R. Surgeon-performed bedside organ assessment with sonography after trauma (BOAST): a pilot study from the WTA Multicenter Group. J Trauma 2005; 59(6):1356-64.
9. Detsky AS, Naglie G, Krahn MD, et al. Primer on medical decision analysis: Part 1–Getting started. Med Decis Making 1997; 17(2):123-5.